Prescription of opioids can sometimes be seen as a requirement in order to guarantee patient satisfaction. Emergency Department (ED) physicians face a difficult challenge when it comes to assessing appropriate management of patients exhibiting “drug seeking” behavior, mainly due to lacking development of continuing medical education and standardized regulatory and legislative protocols. ED physicians were surveyed (n = 141) and 71% reported a perceived pressure to prescribe opioid analgesics to avoid administrative and regulatory criticism. Meanwhile, 98% related patient satisfaction scores as being too highly emphasized by reimbursement entities.

Figure 1: Utilization of opioid abuse identification methods
In Figure 1, the physicians were asked asked about the five methods of opioid abuse identification: physical examination, history, use of the (electronic medical records) EMR, query of the states’ prescription drug monitoring program (PDMP) database, and drug screening. It’s shown that a physical exam, history checks, and use of the EMR are almost always a preferred method amongst physicians in order to identify opioid abuse, however, drug screens seem to be the least utilized method.
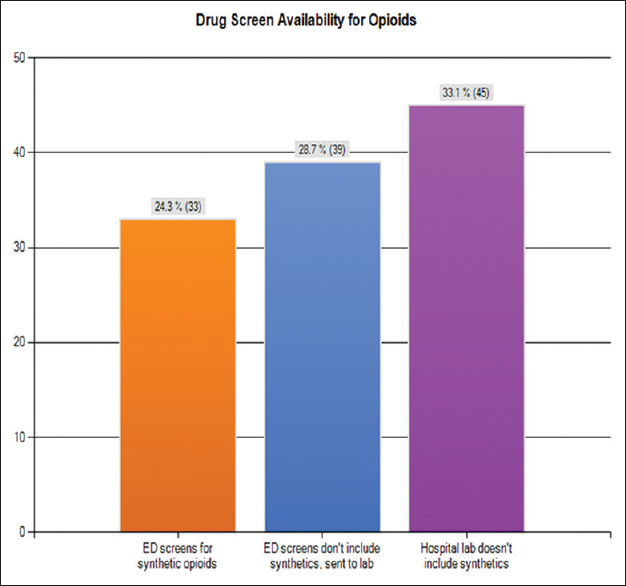
Figure 2: Drug screen availablilty for opioids
Drug screen availability is important when trying to assess a patient who is suspected of opioid abuse, misuse or even of “doctor shopping” for different prescriptions. In Figure 2, only 25% of the respondents had the ability to screen for synthetic opioids in their respective ED's. This limitation could severely impact the ED’s ability to determine a patient’s health status. Testing for synthetic opioids required submission to the hospital laboratory according to 29% of the respondents and 33% had to send samples to an outside laboratory. As mentioned before, this severely limits a physician’s ability to diagnose a patient correctly in order to bring them the best care without accidentally contributing to it in a negative way.
As seen in Figure 1, the use of drug screens for proper diagnostics is rarely employed. Meanwhile, in Figure 2, the drug screening availability seems to be limited in many ED’s. In Figure 3, the participants were asked how regulatory and administrative factors affected their opioid prescribing practices. A majority (72%) felt pressured to prescribe in order to avoid administrative complaints from the patient that pain was inadequately treated.

Figure 3: Perceived pressures to prescribe opioids
Another phenomenon observed in opioid addicts is the so-called “doctor shopping”. What this means is that a person will go to several doctors in order to receive different medications, or to get the response they most want (in this case the prescriptions). Most of the participants stated a lack of clarity on the issue or course of action (Figure 4). An alarming response would be that many (52%) disagree that a failure to report this type of behavior would result in civil liability. Another worrying fact, is that 86% of the participants agreed that hospitals don’t provide protocols for this type of behavior, meaning that there is no established method for dealing with this behavior and there may not be an overall surveillance to make sure that physicians don’t help worsen the condition these patients might be in.

Figure 4: Physician course of action when “doctor shopping” indicated
As seen by Figure 5, most of the participants (98%) believed that patient satisfaction scores should not be used as a metric to assess quality patient care. The heavy weight given to satisfaction scores is a main problem in the opioid epidemic because many patients with opioid addiction, or those who misuse opioids, will give a bad score to any physician who doesn’t meet their demands. In turn, this will make physicians care more about their satisfactory rates and lean more towards overprescribing in order to not get in trouble with their administration.
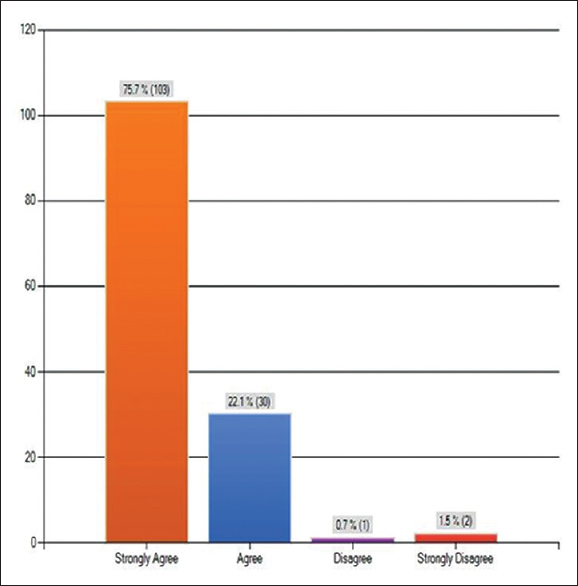
Figure 5: Emphasis on patient satisfaction scores
Overall, the results of this study have identified gaps in training, regulation, and administrative healthcare practices regarding management of patients with a drug-seeking behavior. They’ve also helped to point out many of the attitudes and positions the physicians have themselves regarding the safety and opinion of their patients.