The war on opioids has been an uphill battle since they were marked as a Type 2 Schedule on the Schedule of Controlled Substances according to the Controlled Substances Act of 1970. According to the U.S. Government, drugs in this category have a high abuse potential with severe psychic or physical dependence liability. This is now more clear than ever due to the rampant opioid epidemic that has been going on worldwide. As a means to treat those who have become victims, synthetic opioids have been created which can substitute stronger drugs and eventually be completely eliminated. This allows a person suffering from opioid use disorder to limit or eliminate the drug’s consumption.
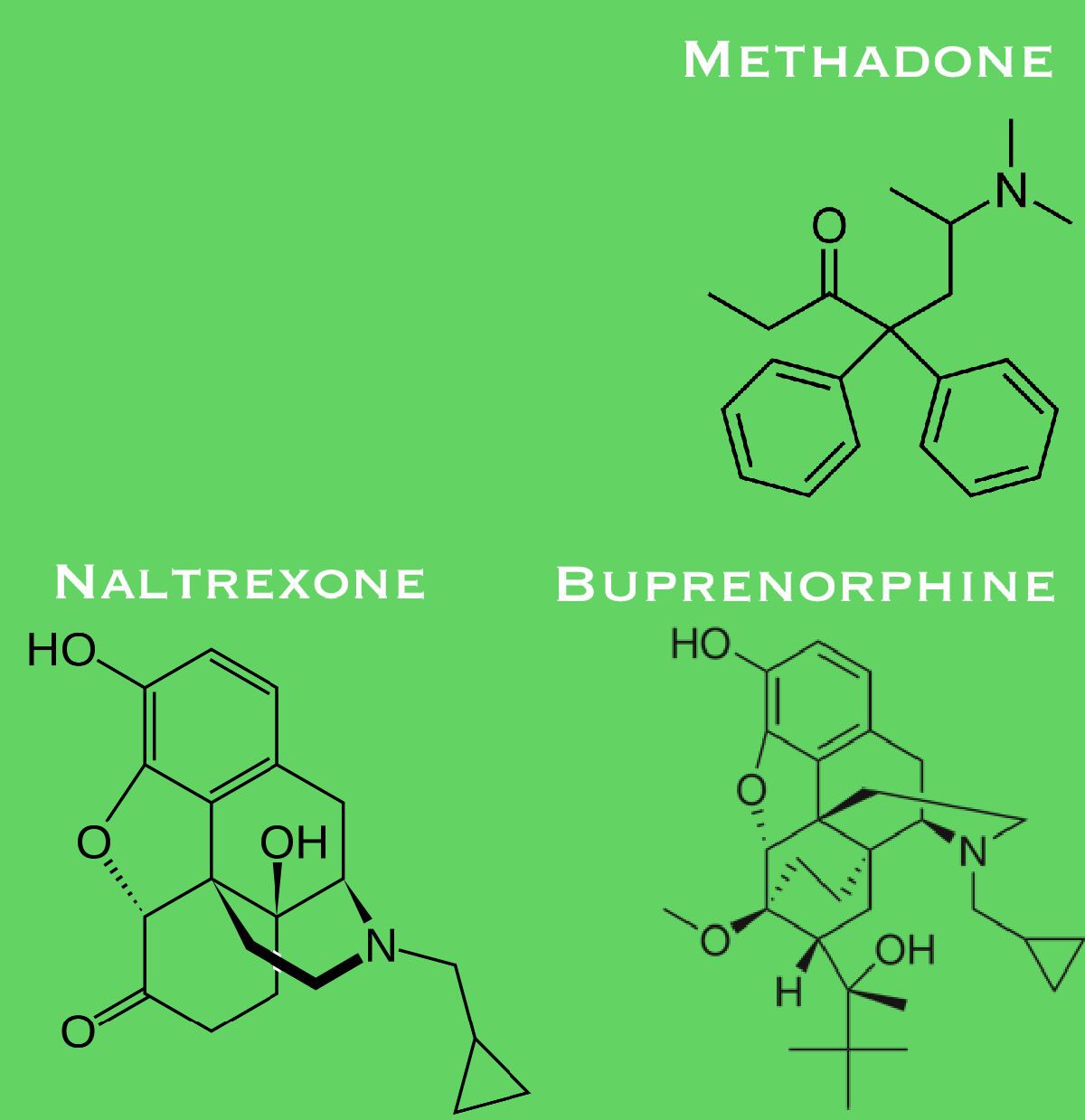
Currently, there are three primary drugs in the medication-assisted treatment such as: methadone, Buprenorphine and Naltrexone. Methadone is an opioid agonist so it is capable of providing the same effects as regular opioids. Yet this drug lasts in the human body for far longer periods of time while providing a weaker analgesic effect than common narcotics which makes it a great option to treat opioid dependence. Buprenorphine is an opioid agonist as well yet it is mainly used when withdrawal symptoms have recently appeared. It can remain in the body even longer than methadone. And lastly, naltrexone is an opioid antagonist which isn't as long lasting as the other treatments but an extended-release version has been created since it has proved to be quite effective.
There are countless studies to address this issue. To better understand the increase in opioid consumption, data has been recollected by different means of people who were suffering from opioid use disorder, people who were under treatment or those whose death was related to opioids.

One study consisted on using carefully selected data from PubMed and Embase databases using keywords related to analyzing them in order to study the effectiveness of the aforementioned opioids as a method of treatment. The methodology to obtain data that could be used to scrutinize the data is presented as Figure 1. The analysis focused on studying the mortality rate of people not receiving any treatment and those who were under treatment yet with different drugs. There were 21 studies focusing on the effects of drug consumption, there was a 0.92 per 100 person-years of crude mortality rate while receiving medicated-assistance, a 1.69 after cessation and a 4.89 for those untreated. There was another analysis done with 16 studies to obtain a clearer conclusion. Based on the crude mortality rate per 100 person-years of the 16 studies, the following conclusions were drawn: there was a 0.24 while receiving medically-assisted treatment, 0.68 after treatment cessation, and 2.43 for those who were untreated. On the 21 studies which focused on all-cause deaths, those who were on MAT with methadone or buprenorphine were 0.93 and 1.79, meanwhile naltrexone were 0.26.
Another statistical analysis provided even more information about the effectiveness of the opioid agonists, buprenorphine and methadone. The databases used were: Cochrane Drugs and Alcohol Review Group, Cochrane Register of Controlled trials, MEDLINE, EMBASE, Current Contents, PsycLIT, CORK, Alcohol and Drug Council of Australia, Australian Drug Foundation, Centre for Education and Information on Drugs and Alcohol and Library of Congress. Through them, it was possible to obtain 31 trials of 5430 participants. The risk ratio was calculated for each treatment at different concentrations (low, medium and high) to see if there was a correlation between the consumption. It was concluded that buprenorphine at any dosage was more effective than the placebo. It was also stated that methadone was more effective in retaining people in treatment than buprenorphine.
No comments:
Post a Comment